Comment on Jun 17, 2020
Amer Zanabili
Dr.

Activities
Comment on Jun 17, 2020
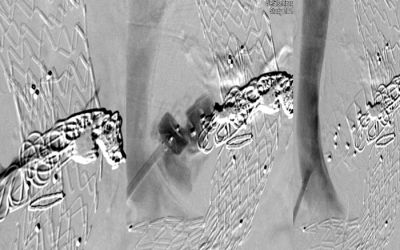
Martin Schroeder commented on presentation CERAB technique in AIOD lesion.
Comment on Jun 16, 2020
Amer Zanabili commented on presentation CERAB technique in AIOD lesion.
Poll 01/06/2019 – 30/06/2019
Vascular Education 2030: One Year Vascupedia
Poll 06/01/2020 – 31/01/2020

VASCUPEDIA@LINC – ENDOLEAKS-CASE-BASED SOLUTIONS
The topic of this month is called ENDOLEAKS-CASE-BASED SOLUTIONS and aims to provide more information to the discussants of the session about endoleaks that will take place on Thursday, January 30, 2020 in Leipzig, during the LINC symposium. Take the opportunity to answer the questions and to inform the experts about your current practice for the treatment of all type of endoleaks.
Your participation will provide unique data for an interesting discussion and your answers will challenge the experts during the session.
Poll 04/10/2019 – 31/10/2019

Choice of antiplatelet therapy around complex revascularisation
A 79-year-old diabetic male patient with no history of coronary disease is referred to you to undergo angioplasty for tissue loss on the tips of the hallux and second toe. He is taking Aspirin 75mg. From preoperative imaging he needs a 20cm SFA occlusion stopping before the adductor hiatus recanalizing as well as multilevel tibial disease which appears to be a combination of short occlusions and stenoses. The dorsal pedal is seen in the foot and is in continuity with the arch. The PT artery appears occluded through it’s whole length.
Poll 05/09/2019 – 30/09/2019
Online education in vascular medicine
Shape your learning experience on Vascupedia
Dear colleagues, our mission is to help physicians worldwide to bring their interventions to perfection. Our hope is to indirectly contribute to safety and well-being of patients with vascular diseases.
Over a year ago, we started Vascupedia as a unique online project that we believe fulfills the need for free education in the challenging field of Vascular Medicine. Now it’s time to ask you to help us to become better for you! Are we offering the right information in the right way at the right level? Is there anything missing to support you in your quest to grow your knowledge to treat your patients in the best possible way? Please complete this short survey to make sure we will work on improving the platform to serve YOUR educational needs!
Poll 01/08/2019 – 31/08/2019
The Type II Endoleak
Patient’s characteristics
Gender: Male
Age: 68 years old
Comorbidity: Arterial hypertension, active smoker
Underwent EVAR 2 years ago
Symptoms: None
DUS/CT A: Aneurysm sac growth > 7mm compared to last CT scan with evidence of type II Endoleak (Inferior mesenteric artery)
Poll 13/04/2018 – 30/06/2018

Topic: Asymptomatic juxta- and pararenal aortic aneurysms
Patient’s characteristics
Gender: Female
Age: 75 years old
Comorbidity: Arterial hypertension, hypercholesterinemia, previous aortocoronary bypass grafting, previous myocardial infarction, previous smoker, peripheral arterial disease, atrial fibrillation
Symptoms: None
Previous operations: None
Aneurysm characteristics:
Max. aneurysm diameter: 54 mm
Length of proximal infrarenal neck: 0 mm
Distance between SMA and LRA: 20 mm
Diameter of renal arteries: RRA: 5,3 mm, LRA: 6 mm
Suprarenal angulation: 60°
Diameter of distal neck: 30 mm
Minimum diameter of common iliac arteries: R: 11 mm, L:9 mm
Maximum diameter of common iliac arteries: R: 11 mm, L: 14 mm
Minimum diameter of external iliac arteries: R: 7 mm, L: 6,2 mm
Poll 01/07/2018 – 31/07/2018

Filiform SFA stenosis – best treatment strategy
Poll 02/02/2019 – 28/02/2019

The acute limb ischemia
Patient’s characteristics
Gender: Female
Age: 65 years old
Comorbidity: Arterial hypertension, Dyslipidemia
Symptoms: Acute onset of claudication (<2 weeks), Rutherford class 3 of the left limb
Previous operations: None
ABI: 0.5
DUS: Occlusion of the left popliteal artery
Poll 02/01/2019 – 31/01/2019

The common femoral artery (CFA) disease
Gender: Male
Age: 73 years old
Comorbidity: Arterial hypertension, hypercholesterinemia, coronary artery disease, previous CABG
Symptoms: Claudication, Rutherford stage 3
Previous operations: None
ABI: 0.5
Poll 01/11/2018 – 30/11/2018

Ilio-femoral deep vein thrombosis
45 years old female patient presenting with painful swelling of the right limb during the last 24 hours. Wells score on admission was 4 points. The duplex ultrasound scanning revealed a femoropopliteal and iliac deep vein thrombosis. No other risk factors were present. No previous operations. No thrombophilia documented.
Poll 01/10/2018 – 31/10/2018

Critical limb-threatening ischemia – CLI Global Society
Patient’s characteristics
Gender: Male
Age: 79 years old
Comorbidity: Arterial hypertension, hypercholesterinemia, chronic kidney disease (GFR: 53 ml/min/1,73m²), NYHA II, Coronary artery disease, previous CABG
Symptoms: Toe ulceration of the left limb
Previous operations: None
ABI: incompressible, Toe pressure: 32 mmHg
Vascular Imaging – Duplex ultrasound: Isolated tibial vessel disease
Poll 01/09/2018 – 30/09/2018

Acute type B aortic dissection
Poll 01/08/2018 – 31/08/2018

Asymptomatic carotid artery disease
Patient’s characteristics
Gender: Female
Age: 72 years old
Comorbidity: Arterial hypertension, hypercholesterinemia, previous smoker
Symptoms: None
Previous operations: None
Vascular Imaging of the left internal carotid artery: Duplex ultrasound with peak systolic velocity (PSV)> 230 cm/sec
Poll 01/08/2018 – 31/08/2018
Asymptomatic carotid artery disease
Patient’s characteristics
Gender: Female
Age: 72 years old
Comorbidity: Arterial hypertension, hypercholesterinemia, previous smoker
Symptoms: None
Previous operations: None
Vascular Imaging of the left internal carotid artery: Duplex ultrasound with peak systolic velocity (PSV)> 230 cm/sec
Poll 01/03/2019 – 31/03/2019

The chronic mesenteric ischemia
Patient’s characteristics
Gender: Female
Age: 69 years old
Comorbidity: Arterial hypertension, Dyslipidemia, coronary heart disease (DES deployment 2 years ago)
Symptoms: Postprandial pain
Previous abdominal operations: None
DUS: Occlusion of the superior mesenteric artery